

















































Nigeria’s Real and Growing Commitment to the Early Years
Nigeria has made meaningful, deliberate investments in the early years of its children’s lives. The National Policy on Education formally recognises Early Childhood Care and Development (ECCD) as a foundational phase of the education continuum. The National Policy on Integrated Early Childhood Development provides a framework for multi-sectoral action. The Basic Healthcare Provision Fund (BHCPF) has expanded community health access to millions of families. The National Primary Health Care Development Agency (NPHCDA) has deployed a nationwide network of Community Health Extension Workers (CHEWs) as the front line of child and maternal health services. State governments in Lagos, Anambra, Kaduna, and others have invested in ECCD centres, parenting programmes, and community-level health and nutrition integration. These are not small achievements. They represent the determined effort of government, communities, and partners to give Nigeria’s youngest citizens the start they deserve.
At the same time, Nigeria’s leaders, educators, and health professionals are rightly asking a deeper question: how do we make these investments work together more powerfully? With over 30 million children under five, Nigeria has both the scale of ambition and the urgency of need to move from strong individual programmes to a truly integrated system. A system where every child from birth to six years is reached by health, nutrition, stimulation, and support that work in concert rather than in isolation. This article explores how a convergence approach can help Nigeria unlock the full potential of the foundations it has already built.
‘Nigeria’s commitment to its youngest children is real and growing. The next step is weaving its strong programmes into a system that reaches every child as a whole.’
The Power of Integration: Why Convergence Matters
Ninety percent of a child’s brain development occurs before the age of five. In those critical early years, a child’s nutritional status, the richness of language they hear at home, the security of their emotional bonds, their physical health, and whether any developmental challenge is identified early. All of these shape their capacity to learn for the rest of their life. These dimensions of development do not happen in sequence. They happen simultaneously, and they strengthen each other when supported together.
This is the insight at the heart of a convergence model: that a child does not experience life in sectoral silos, and the system serving that child should not be organised in them either. When a community health worker who visits a mother also provides early stimulation guidance, checks the infant’s developmental milestones, and connects the family to a preschool readiness programme as the child turns three, the impact is not merely additive. It is transformative. Nigeria already has many of the building blocks of this integrated vision. The opportunity is to bring them together into a coherent architecture that multiplies their combined effect.

Global Best Practice: Lessons from India’s ICDS Experience
Among the global models of integrated early childhood programming, India’s Integrated Child Development Services (ICDS) offers instructive lessons. This is not as a blueprint to copy, but a rich source of learning about what convergence looks like in practice at scale. Launched in 1975 and now reaching over 100 million beneficiaries, ICDS is built around one central idea: that a single community-level hub, staffed by a trained worker, can deliver six integrated services to children and families simultaneously.

The ICDS model places an Anganwadi worker at the heart of each community hub. From this single convergence point, she delivers: supplementary nutrition to children and pregnant or nursing mothers; health checkups and growth monitoring; immunisation coordination; referral of children who need specialist support; pre-school education and early stimulation for children aged three to six; and parenting and nutrition education for caregivers. Crucially, the model integrates governance too- the Ministries of Women and Child Development, Health, and Education share accountability through a common framework rather than operating in separate administrative lanes.
What makes ICDS particularly relevant for Nigeria is not its size but its architecture. The principle of a multi-thematic community touchpoint, a trained convergence worker, and shared governance across sectors is one that Nigeria is already partially implementing through its CHEW cadre and PHC infrastructure. ICDS demonstrates that when these elements are coordinated and empowered together, they produce outcomes far greater than any single programme can achieve alone.
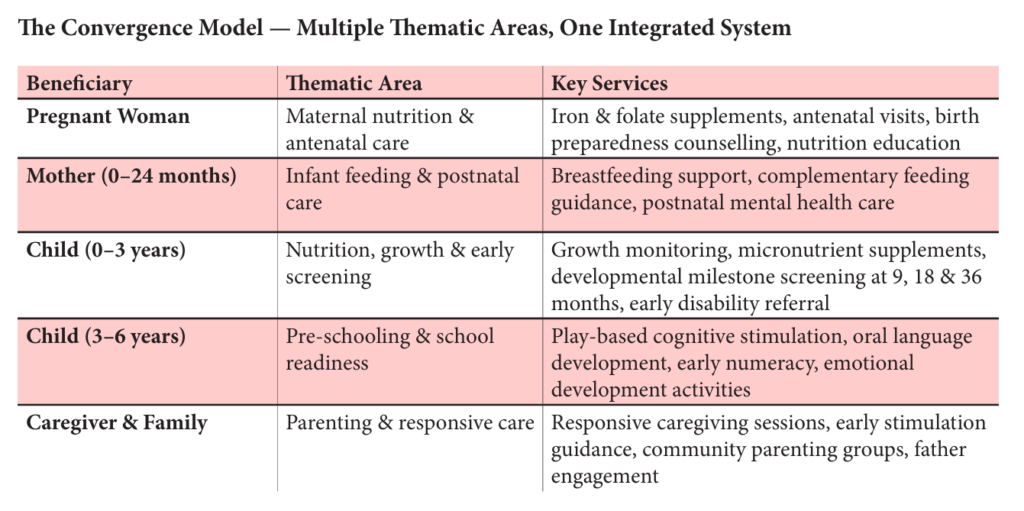
The Convergence Model — Multiple Thematic Areas, One Integrated System
Six Thematic Pillars for Holistic Development
A convergence model for children aged zero to six rests on six interconnected pillars. Nigeria’s existing programmes and infrastructure already engage each of these areas. The goal of convergence is to strengthen the links between them so that every child benefits from all six, delivered in coordination:
Maternal and Child Nutrition. Nigeria’s National Guidelines on Infant and Young Child Feeding and the ongoing National Home Fortification Programme reflect a strong policy commitment to child nutrition. The convergence model builds on this by embedding nutrition support from prenatal supplementation through complementary feeding guidance, within the same community touchpoint that delivers stimulation and health services, so that a mother never has to choose between appointments.
Pre-schooling and Cognitive Development. Nigeria has invested in ECCD centres across states, and the Universal Basic Education Commission has worked to formalise early learning structures. A convergence approach extends this by bringing play-based stimulation and language-rich activities into community health spaces for children aged zero to three (the years before formal preschool enrolment), closing the gap that currently exists between health visits and structured early learning.
Physical Development. Nigeria’s Immunisation Programme, managed through the NPHCDA, is one of the continent’s most extensive. The CHEW-based Ward Health System already conducts growth monitoring visits. Convergence means using these touchpoints to also track motor development milestones, so physical and developmental health are assessed together in a single, family-friendly interaction.
Emotional and Social Development. Responsive, warm caregiving is the neurological foundation for all learning and social competence. Nigeria’s strong family and community networks including faith communities and women’s groups, are natural channels for structured parenting support programmes. Community Health Extension Workers can be equipped to facilitate these sessions as part of their routine visit, transforming what is already a trusted relationship into a vehicle for emotional development support.
Early Identification of Disability and Developmental Delays. This is an area of significant global opportunity that Nigeria is well-positioned to advance. When developmental screening is embedded in routine child health contacts at nine, eighteen, and thirty-six months, children with hearing impairments, vision challenges, speech delays, or other developmental needs are identified early during the window when intervention is most effective. Nigeria’s existing referral infrastructure, including State Specialist Hospitals and tertiary health centres, can serve as the receiving end of a strengthened community-to-specialist pathway.
School Readiness. School readiness is not a separate programme. It is the natural outcome of a child who has been well-nourished, stimulated, kept healthy, emotionally supported, and seen fully by the system around them. Nigeria’s investment in the transition from ECCD to primary school, including the Grade 1 readiness agenda within UBE, is strengthened enormously when the convergence system upstream has done its work in the years from birth to six.
Building on Nigeria’s Strong Foundations: Nigeria does not need to start from scratch to build a convergence system. It needs to recognise, connect, and amplify what it already has. The CHEW cadre i.e over 50,000 trained community health workers deployed across wards, which is one of Africa’s most extensive community health workforces. The PHC network, revitalised through the BHCPF, provides the physical infrastructure for community-level convergence hubs. The Saving One Million Lives programme demonstrated that targeted, evidence-based investment in community health workers produces measurable results in child survival and maternal health. State-level innovations, particularly in Lagos, Anambra, Ogun, and Kaduna, show what integrated early childhood delivery can look like when political will and community trust are aligned.
What the convergence model asks of Nigeria is not to replace these assets but to connect them more deliberately: to train community workers across the full spectrum of early childhood domains, to establish shared accountability frameworks across the relevant federal ministries, to embed developmental screening systematically into existing health contacts, and to use the community spaces already trusted by families as the anchor points for integrated service delivery. India’s ICDS experience shows this is achievable. Nigeria’s own track record shows it has the human resource, the infrastructure, and the community relationships to make it work.
Strengthening the System: Six Practical Steps
Unite the governance. Establish a formal inter-ministerial ECD coordination mechanism spanning Women Affairs, Health, and Education, building on Nigeria’s existing Federal Executive Council structures, so that ECCD outcomes are owned collectively and accountability is shared.
Empower community convergence hubs. Designate existing PHC centres and ward health posts as integrated ECD service points, with expanded scope to deliver nutrition, stimulation, screening, and parenting support under one roof, maximising the value of infrastructure that communities already use and trust.
Invest in the CHEW as a convergence worker. Expand CHEW training to include early stimulation, play-based learning facilitation, developmental screening tools, and responsive caregiving support, reflecting the full breadth of the early childhood mission and rewarding workers accordingly.
Embed developmental screening in the child health schedule. Integrate milestone checks at nine, eighteen, and thirty-six months into routine CHEW visits, with clear referral pathways to district health facilities and specialist centres, so that early identification of developmental needs becomes standard practice rather than an exception.
Build a unified child record. Link birth registration, nutrition records, immunisation data, developmental screening results, and ECCD enrolment into a single longitudinal profile for each child, giving the system visibility across domains and enabling targeted support for those who need it most.
Harness Nigeria’s social capital. Community parenting programmes, delivered through the faith institutions, market women’s associations, ward development committees, and community leaders that already hold trust in Nigerian communities, are among the highest-leverage investments the system can make. These channels can carry the message of responsive caregiving, early stimulation, and nutritional support to families in the language and relationships they already inhabit.
A Chapter Nigeria Is Already Writing Nigeria’s commitment to its youngest citizens is visible in its policies, its programmes, and the daily work of thousands of CHEW staff, ECCD workers, health professionals, and community volunteers across the country. The convergence model is not a verdict on what Nigeria has failed to do. It is a framework for amplifying what Nigeria has already built by bringing its strong but separate strands of work into a more coherent, integrated system that reaches every child in the critical years from birth to six.
The global evidence, and the ICDS experience in particular, shows that when health, nutrition, early stimulation, emotional development, and disability identification are delivered as a coordinated whole rather than isolated programmes, the impact on children’s development, school readiness, and long-term outcomes is transformative. Nigeria has the foundations, the workforce, and the community networks to realise this vision. The next chapter in Nigeria’s early childhood story is one this country is entirely capable of writing and the children who will benefit from it are waiting.
‘Nigeria has the foundations, the workforce, and the community trust to build an integrated early childhood system. The convergence model is not a new direction; it is the next step on a journey already underway.’
____________________

Shashank Khare is a development professional based in India with over 14 years of experience advancing systemic reforms in school education and Early Childhood Care and Development (ECCD). He has led large-scale government-partnered initiatives to strengthen foundational learning, integrate digital pedagogy, and build data-driven decision-making systems in the public education sector, with a strong focus on ecosystem convergence, multi-stakeholder coordination, and sustainable scale within government systems.
LinkedIn: www.linkedin.com/in/shashank25khare | Email: Sk.khare25@gmail.com